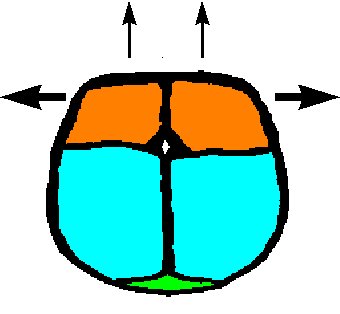
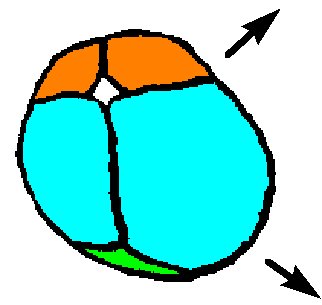
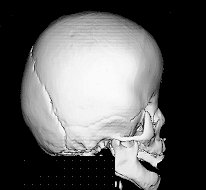
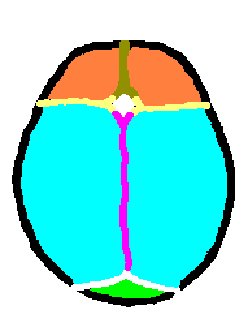
 The calvarium is divided by sutures into bony plates. In this illustration,
the brown metopic suture divides the orange frontal bones.
The frontal bones are separated from the blue parietal bones by
the yellow coronal suture, and the two parietal bones are separated
from each other by the purple sagittal suture. The occipital
bone is separated from the parital bones by the white lambdoidal
sutures. The space where the metopic, coronal and sagittal sutures
come together is the anterior fontanelle, and the posterior fontanelle
is present where the lambdoidal and sagittal sutures meet.
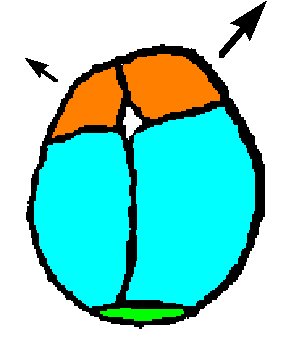
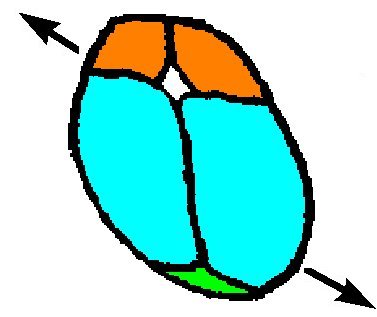
The calvarium is divided by sutures into bony plates. In this illustration,
the brown metopic suture divides the orange frontal bones.
The frontal bones are separated from the blue parietal bones by
the yellow coronal suture, and the two parietal bones are separated
from each other by the purple sagittal suture. The occipital
bone is separated from the parital bones by the white lambdoidal
sutures. The space where the metopic, coronal and sagittal sutures
come together is the anterior fontanelle, and the posterior fontanelle
is present where the lambdoidal and sagittal sutures meet.
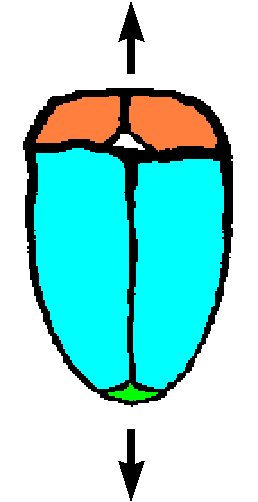
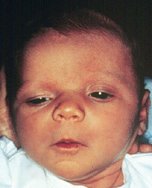
- most common, 58% of all synostoses
- 2-3 x more males than females
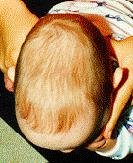
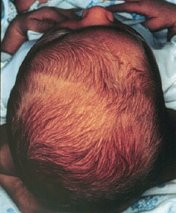
- dolichocephalic/scaphycephaly (long-headed/keel-headed)
- May be turricephalic (tower-headed)
- frontal and/or occipital bossing may be present
- frequently, early closure of anterior fontanelle
- about 10% associated with increased ICP
shape complicates vaginal delivery